
Case Scenario: Fall and Possible Hip Fracture in a Long‑Term Care Resident
1. Resident Background
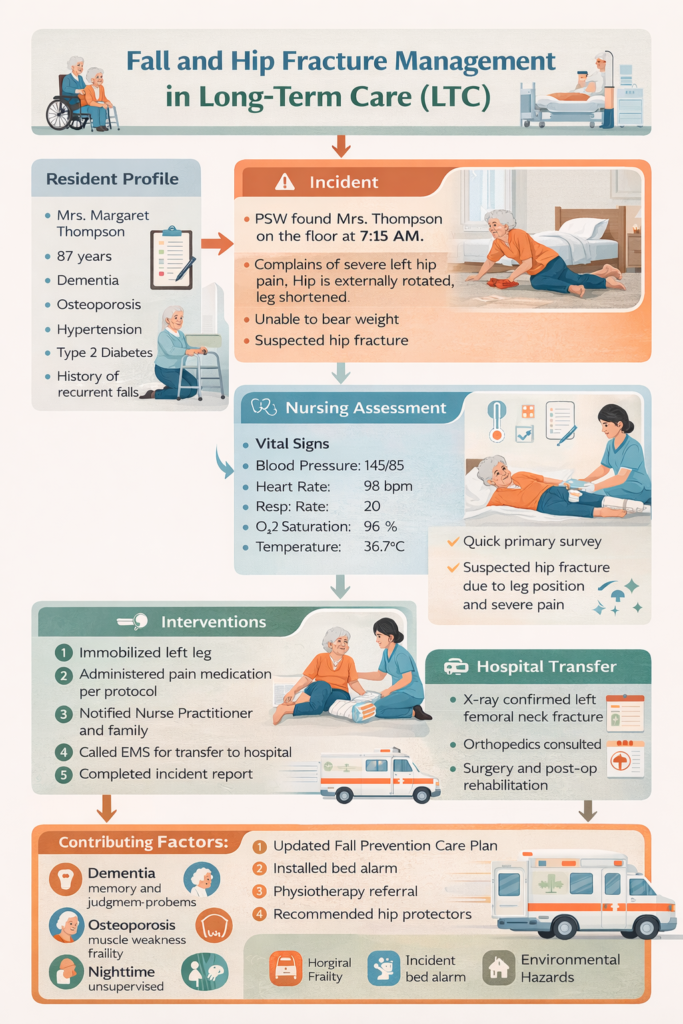
Mrs. Margaret Thompson is 87 years old, lives in a long-term care home, and has multiple risk factors for falls:
- Dementia: Cognitive impairment increases risk of wandering, poor judgment, and delayed reporting of discomfort. Residents may attempt independent mobility without realizing danger.
- Osteoporosis: Fragile bones make fractures more likely even with minor trauma.
- Hypertension & Diabetes: Chronic conditions may contribute to fatigue, balance issues, or peripheral neuropathy.
- History of Falls: Previous falls are a strong predictor of future falls.
Understanding the resident’s medical history and functional abilities is critical in both prevention and post-fall care.
2. Incident Description
The fall occurred early in the morning, which is a high-risk time in LTC:
- Residents may wake disoriented, attempt to go to the bathroom independently, or struggle with night-time lighting.
- Mrs. Thompson was found on the floor, indicating that the fall was unwitnessed, which is common in LTC homes.
- Initial observations included pain, leg rotation, and shortening—classic signs of a hip fracture, which are urgent medical concerns.
Clinical Importance: Falls in elderly residents are high-risk events that can lead to hospitalization, loss of mobility, and even increased mortality.
3. Nursing Assessment
The primary assessment followed standard clinical protocols:
- Airway, Breathing, Circulation (ABC)
- Ensured no immediate life-threatening compromise. Vital signs were stable: BP 145/85, HR 98, RR 20, O2 sat 96%.
- Physical Examination
- Noted tenderness, leg shortening, and external rotation, all signs indicative of femoral neck fracture.
- Checked for other injuries: head trauma, lacerations, skin integrity.
- Pain Assessment
- Pain scored 8/10, prompting timely pain management per protocol.
- Fall Risk Evaluation
- Reviewed history and contributing factors for the incident.
Clinical Reasoning: A careful assessment differentiates between minor injuries and serious fractures requiring hospitalization.
4. Nursing Interventions
Immediate interventions focus on safety, pain management, and preventing complications:
- Immobilization: Stabilized the leg to avoid further injury during transport.
- Minimal Movement: Avoided lifting or repositioning the resident unnecessarily.
- Pain Management: Administered analgesics as per standing orders or physician direction.
- Neurological Monitoring: Checked for signs of head injury.
- Physician Notification: Alerted NP/physician to review and order further treatment.
- EMS Activation: Coordinated hospital transfer safely.
- Documentation: Detailed recording of vitals, interventions, and incident timeline.
Team Coordination: Other staff assisted by monitoring nearby residents, preparing documentation, and supporting communication with family.
5. Communication
Clear and structured communication is critical:
- Family: Informed immediately to reduce anxiety and ensure informed consent.
- Hospital Staff: Provided history, medications, and incident details for continuity of care.
- Internal Documentation: Included in incident report and care plan review.
Clinical Significance: Proper communication ensures timely medical intervention and prevents medical errors.
6. Hospital Outcome
- X-ray confirmed a left femoral neck fracture, a common consequence of falls in elderly residents with osteoporosis.
- Surgical intervention (hip pinning or replacement) was required, followed by post-operative rehabilitation.
Learning Point: Early recognition and hospital transfer prevent further complications, such as prolonged immobility, pressure ulcers, and infections.
7. Root Cause Analysis
Falls are usually multifactorial:
- Cognitive decline from dementia → wandering, impulsivity.
- Weakness or balance impairment → inability to stabilize during a misstep.
- Environmental hazards → poor lighting, clutter, slippery floors.
- Medication side effects → dizziness, hypotension, hypoglycemia.
Clinical Application: LTC staff must assess both intrinsic (resident-related) and extrinsic (environment-related) risk factors for fall prevention.
8. Prevention Strategies
The LTC home implemented evidence-based strategies:
- Enhanced Fall Risk Care Plan → individualized interventions.
- Bed and chair alarms → alert staff when a high-risk resident attempts to move.
- Nighttime supervision → regular checks during vulnerable hours.
- Hip Protectors → reduce fracture severity during falls.
- Physiotherapy/Strengthening Programs → improve mobility and balance.
Outcome: Fall prevention requires interdisciplinary collaboration—nurses, PSWs, physiotherapists, and physicians working together.
9. Why This Case is “Frequent” in Ontario LTC
- Falls are the most common adverse events in LTC homes.
- Residents with dementia and osteoporosis are particularly vulnerable.
- Early morning hours and unsupervised mobility are high-risk scenarios.
- Hip fractures lead to hospitalization, rehabilitation, and significant functional decline.
Key Learning: LTC nurses must anticipate fall risks, respond quickly, and coordinate care efficiently.
10. Lessons for Nursing Practice
- Rapid Assessment: Always perform a thorough primary and secondary assessment.
- Pain & Safety First: Immediate pain relief and immobilization reduce further injury.
- Effective Communication: Notify physician, family, and EMS promptly.
- Documentation: Detailed records protect residents and staff legally.
- Preventive Measures: Evaluate the resident and environment to prevent future falls.
- Interdisciplinary Approach: Collaboration is essential for comprehensive care.
Clinical Analysis: Fall and Possible Hip Fracture in LTC
1. Clinical Significance
Falls are one of the most frequent and high-risk incidents in long-term care homes in Ontario, particularly among residents with:
- Advanced age
- Cognitive impairment (dementia)
- Osteoporosis or frailty
- History of previous falls
In this case, the fall was unwitnessed, yet rapid assessment by nursing staff identified classic signs of a hip fracture (leg shortening, external rotation, and severe pain). Early recognition was critical to:
- Prevent further injury
- Initiate timely pain management
- Enable safe hospital transfer
2. Nursing Assessment and Critical Thinking
The RN followed a structured assessment:
- Primary survey (ABCs) ensured no immediate life-threatening compromise.
- Vital signs indicated relative stability, but monitoring was essential for shock or bleeding.
- Physical assessment detected hip deformity and tenderness, prompting suspected fracture.
- Pain assessment (8/10) guided administration of analgesics.
Analysis:
The nurse’s ability to differentiate between minor fall-related injury and potentially serious fractures highlights the importance of clinical judgment in LTC, especially when dealing with frail, elderly residents.
3. Nursing Interventions
Key interventions included:
- Immobilization of the affected limb to prevent additional injury.
- Minimal movement of the resident until EMS arrival.
- Pain management per protocol.
- Notification of physician/NP and family.
- Hospital coordination for safe transfer.
- Documentation of vital signs, assessment findings, and interventions.
Analysis:
These interventions reflect adherence to evidence-based fall and fracture management protocols in LTC. The structured approach ensures resident safety, comfort, and continuity of care.
4. Communication and Teamwork
Effective communication was critical:
- Internal communication: PSWs alerted the RN immediately.
- Physician/NP notification: Provided complete incident details, vitals, and assessment findings.
- Family notification: Maintained transparency and trust.
- EMS handoff: Smooth transition ensured continuity of care and minimized delays.
Analysis:
This case demonstrates that team coordination and communication are essential to prevent adverse outcomes in fall-related incidents.
5. Root Cause and Preventive Analysis
Factors contributing to the fall included:
- Cognitive impairment → poor judgment and unsafe mobility
- Physical weakness → difficulty stabilizing during movement
- Environmental factors → potential hazards, low lighting
- Polypharmacy → increased risk of dizziness or hypotension
Analysis:
Falls are multifactorial, requiring both resident-centered strategies (exercise, hip protectors, cognitive monitoring) and environmental modifications (lighting, alarms, removal of tripping hazards).
6. Lessons Learned
- Early Recognition: Staff should be vigilant for high-risk residents, especially in the early morning or during routine mobility.
- Structured Assessment: Use systematic assessment (vitals, pain, injury signs) to differentiate minor vs. serious injuries.
- Prompt Intervention: Immobilization, pain management, and timely physician notification prevent complications.
- Team Communication: Clear handoff to EMS and hospital staff ensures continuity of care.
- Fall Prevention Planning: Post-fall, implement environmental modifications, physiotherapy, alarms, and protective equipment.
- Documentation and Reporting: Accurate documentation supports legal compliance, quality improvement, and future risk mitigation.
- Emotional Support: Residents and staff benefit from debriefing after high-stress events, reducing trauma and burnout.
7. Clinical Implications for LTC Nursing
- LTC nurses must be proactive in assessing fall risk and implementing preventive measures.
- Rapid recognition and structured response save lives and reduce morbidity.
- Interdisciplinary collaboration (nurses, PSWs, physiotherapists, physicians) is essential for effective management.
- Continuous education and simulation training in fall management improve staff preparedness.
8. Conclusion
The case of Mrs. Thompson highlights a frequent, high-stakes scenario in Ontario LTC homes. Through timely assessment, coordinated interventions, and structured communication, serious complications were minimized. Nursing staff must remain vigilant, proactive, and collaborative to ensure safety, prevent injury, and maintain high-quality care in long-term care settings.